Why Are Private Hospitals so Expensive in Venezuela?
The collapse of public healthcare and medical supplies production are two of the main elements which lead in how costs pile up in the private health sector
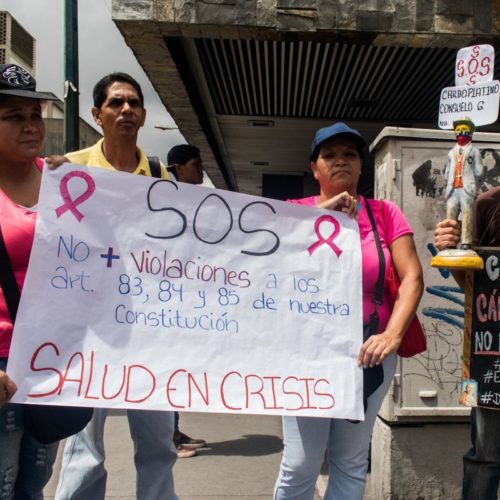
Photo: Sofía Jaimes Barreto
The sustained decline of public hospitals in Venezuela is still ongoing, and private hospitals are still the way to go if you want efficient medical attention—as long as you have over $40 for a doctor’s visits, over $1,000 (daily) if hospitalization is needed, and over $3,500 for basic medical procedures.
This is in a country where the real value of the minimum wage is under one dollar.
With these estimated costs, private health care has become unaffordable for most Venezuelans, one of the most terrible consequences of the country’s macroeconomic crisis and of many other issues that overlap, constituting the complex humanitarian emergency.
From Public Health Care Decline to Depending on the Private Sector
Towards the end of the 1950s, public health care services in Venezuela began deteriorating, and this led to a rise in the number of private institutions offering services of higher quality.
Pedro Delmédico, former president of the Asociación Venezolana de Clínicas y Hospitales (Venezuelan Association of Clinics and Hospitals), explains: “By 1999, along with a decentralization that wasn’t very well regulated and resulted in some states having much better public health care services than others, there was a slow and continuous drop in investment of the GDP in health care, which peaked between 2003 and 2005.” Public investment went to the Barrio Adentro chavista system, to build and equip walk-in clinics, diagnostic centers, and rehabilitation halls in poorer and rural areas of Venezuela. With the exception of the Hospital Cardiológico Infantil, the program focused on primary health care. Older clinics and hospitals, even fourth tier ones (which include general surgery services) continued to suffer with poor investment, even for the replacement of medical supplies, maintenance, and updates on equipment.
The salary improvement for health care staff also began to wane, to the benefit of Cuban doctors brought in to lead medical attention in the Barrio Adentro system. Venezuela, as a host country, still pays for this service to the Cuban government.
At least 80% of medical supplies in a private hospital are imported, so without subsidized dollars you can’t have reasonable prices.
The seriousness of it all is that “when hospitals became more expensive, all other medical services were affected,” Delmédico points out, and due to the lack of efficient public health care alternatives, patients had to shift to the private health sector, either because they could afford it or because they had health insurance.
Private hospitals were now tending to the growing demand of patients while looking to stay up to date in the use of new medical technology. They achieved this by having access to subsidized dollars, which had become unaffordable between the years 2000 and 2015.
From Subsidized Dollars to Spontaneous Dollarization
At least 80% of medical supplies in a private hospital are imported, so without subsidized dollars you can’t have reasonable prices. On the other hand, without those preferential dollars, purchasing supplies is also hindered: laboratories, supply stores, and international distributors have closed down in Venezuela. Having fewer brands leads to less competition and more speculation.
So, between 2015 and 2018, buying any supplies needed for patients became a complicated issue. Eduardo Mathison, economist and former president of the Centro Médico Docente La Trinidad, a private hospital in Caracas, explains: “Today, for instance, if you have to bring a new piece of equipment from abroad, it means dealing with a terrible speculation chain. The manufacturer, the provider isn’t in on it. He sells it to the area’s exclusive distributor and then it begins: if you want that distributor to get you the permit, you have to give him a little extra. And then to the next guy to let it go through customs, and then to another guy who allows it to enter, and another one to release it. All of this on top of shipping and duties.”
In other words: private hospitals are the second to last affected in the consumer chain.
From the moment a product leaves its country of origin to be used on a patient in Venezuela, its cost is always increasing for the profit of distributors and agents, and it turns into an unattainable commodity for the patient.
The only way for a Venezuelan hospital to recoup the investment made on any supply is by charging the final cost to the patient through cash flow, since credits are not only scarce, but not high enough to cover such high amounts.
The economic sanctions established and led mostly by the United States don’t include health sanctions; there are sanctions on oil, not on health services.
Investing in medical technology, be it in equipment, basic supplies, medicine, research and training healthcare professionals, is necessary and unavoidable when you want to provide efficient, high-quality service which also allows for improvement in medical attention.
As Mathison points out, health is expensive, because the technology is expensive to purchase, maintain and replace.
Neither the Doctor Nor the Sanctions Are to Blame
The Constitution and the law for practicing medicine in Venezuela allow for doctors to establish their fees in agreement with the patient and the medical facility where they work. Fees vary but, as Delmédico warns, “the difference in price has to be in context: costs are more or less the same in A-level hospitals, which have all the technologies. We obviously can’t compare an A hospital with a C hospital, which is smaller, so the costs differ. But be it in either A or C, no one’s exempt from specialized attention, defensive medicine, which is why the patient is asked to have many tests done, to avoid missing something and protect ourselves from malpractice lawsuits. This, of course, is an important component in the patient’s bill.”
When it comes to sanctions, Mathison clears things out: “They have nothing to do with it. Whoever claims it does is very irresponsible. The economic sanctions established and led mostly by the United States don’t include health sanctions; there are sanctions on oil, not on health services.”
Dollarization Isn’t the Cure
The decision by the Venezuelan Central Bank regarding foreign currency control allows for a transaction economy, but the macroeconomic distortion persists and still affects us: “Since the end of 2019, the supply of medical materials and medicine has improved, because you can buy and sell in dollars, but there’s been a change in how many products and services you can pay for with those dollars: what you could buy with $30 or $33 in January 2020, now costs $100,” Delmédico explains.
But invoices from private hospitals don’t show much profit. Since 2014, and even today with a consolidated hyper-inflation, the SUNDDE (the institution in charge of price controls and enforcing business compliance with government regulations) supervises, audits and makes sure that health care facilities don’t exceed 30% in earnings, even though only replacing medical supplies costs much more than that. As Delmédico says, “You have hyperinflation and excessive controls,” along with private property and economic freedom rights being violated.
To maintain profitability in a private hospital means, on top of everything, to sustain a payroll which represents around 40% of the costs, as well as complying with other obligations: payments of between 18 and 22 taxes and basic services which, even after being charged in dollars, have increased their fees.
“Yes, private hospitals are expensive, but if you go deeper, you realize that, when possible, the profitable cost tries to offer a service within reach of the people. We have to say it: private hospitals are a service intended for taxpayers, and the State should provide for their health care, which is a basic need and a universal human right that they don’t have,” Delmédico concludes.
Caracas Chronicles is 100% reader-supported.
We’ve been able to hang on for 22 years in one of the craziest media landscapes in the world. We’ve seen different media outlets in Venezuela (and abroad) closing shop, something we’re looking to avoid at all costs. Your collaboration goes a long way in helping us weather the storm.
Donate